Phenylephrine (PE), a common ingredient in oral nasal decongestants, may provide no more relief for stuffy noses than a placebo, according to the unanimous decision of the U.S. FDA expert panel. In Nigeria, PE is available in several cough & cold combination products namely:
Phenylephrine gained prominence in over-the-counter decongestants after pseudoephedrine, an older ingredient, was moved behind pharmacy counters due to its potential for illegal processing to methamphetamine. Phenylephrine became the leading over-the-counter alternative, labeled as “PE.”
The FDA’s re-evaluation was triggered by researchers from the University of Florida, who petitioned for the removal of phenylephrine products based on recent studies showing their ineffectiveness compared to placebo pills in patients with cold and allergy congestion. These researchers previously challenged the drug’s efficacy in 2007, but it remained on the market pending further research, as recommended by FDA experts at the time.
This time, the FDA panel of 16 members unanimously concurred that current evidence does not support the drug’s effectiveness. The panel echoed the findings of an FDA scientific review published before the meeting, which identified significant flaws in the small studies from the 1960s and 1970s that originally led to phenylephrine’s approval. These studies used outdated statistical and research techniques no longer endorsed by the agency.
Moreover, three more recent and rigorously conducted studies, conducted by Merck and Johnson & Johnson after 2016, found no discernible difference between phenylephrine medications and placebos in relieving congestion.
FDA reviewers believe that their latest assessment reflects new insights into how quickly phenylephrine is metabolized when taken orally, resulting in only trace levels reaching nasal passages to alleviate congestion. The drug appears to be more effective when applied directly to the nose in the form of sprays and drops.
Alternative remedies are available: Some nasal decongestants, such as sprays containing phenylephrine, can still be effective for short-term use. Other options include nasal saline rinses, humidification, drinking water and honey. Consumers should consult their pharmacists for the best advice.
Popular nasal decongestant doesn’t actually relieve congestion, U.S. FDA experts say [Internet]. Medical Post. 2023 Sep 12 [cited 2023 Sep 14]. Available from: https://www.canadianhealthcarenetwork.ca/ (login required)
It doesn’t and shouldn’t based on the findings of a 2015 UK study on sexuality among older adults.
Sexual activity among seniors is often underestimated and overlooked by society and medical professionals. There are biases that associate sex with youth and fertility, leading to the neglect of the sexual lives of older individuals. However, research indicates that sexuality remains important for people of all ages and has various physical, emotional, and relational benefits.
The data from the UK study revealed that while there is a decline in sexual activity with age, it does not disappear entirely. Among men aged 70-79, 59% reported having had sex in the past year, with 19% engaging in intercourse at least twice a month and 18% masturbating with similar frequency. The numbers dropped to 39%, 6%, and 5%, respectively, for men above the age of 80. The reasons behind these declines include societal taboos, fear of disease, medications or interventions affecting sexual function, disfigurement, and the natural effects of aging.
For women aged 70-79, 39% reported having had sex in the past year, with 6% engaging in intercourse at least twice a month and 5% masturbating with similar frequency. Among women above the age of 80, these numbers dropped to 10%, 4.5%, and 1%, respectively. Factors affecting women’s sexual activity mirrored those of men, along with the unfortunate reality that many heterosexual women become widowed as their older male partners pass away.
The differences in sexual activity between men and women can also be attributed to lower levels of testosterone in women. Additionally, women tend to prioritize intimacy over performance, which may explain their lower frequency of masturbation. It is important to note that intimacy can be experienced without engaging in intercourse or masturbation.
How can healthcare professionals help older adults with their sexuality?
Healthcare professionals can help older adults with their sexuality by being more proactive in asking about it. Clinicians rarely ask about sexuality and this failing can be harmful. By being more open and willing to discuss sexuality with their older patients, healthcare professionals can help to address some of the biases and taboos surrounding this topic and improve the quality of life for their patients.
In conclusion, older adults continue to engage in sexual activity, although at lower frequencies compared to younger individuals. Recognizing and addressing the sexual needs and concerns of older patients is crucial for their overall quality of life.
Source:
Gianotten, W. L. (2023, May 18). No Expiration Date for Sex! Medscape Family Medicine. WebMD LLC
The National Agency for Food and Drugs Administration and Control (NAFDAC) has issued a public alert on the recall of two lots of Norvasc 5mg tablets. The recall was ordered by the Taiwan Food and Drug Administration (FDA) after the discovery of iron wires in samples taken from a shipment of six million tablets produced by U.S.-based drug developer Viatris Inc. Long-term local Norvasc users have also reported finding iron wires inside the tablets.
Norvasc 5mg tablets contain amlodipine besylate, which is used to treat high blood pressure or angina.
The affected batches are FR3135 and FT2343 – see the image below.
NAFDAC advises importers, distributors, retailers, and consumers to exercise caution and vigilance within the supply chain to avoid importing, distributing, selling, or using these affected batches.
Members of the public in possession of these products are advised to discontinue sale or use and submit stock to the nearest NAFDAC office. If you have used these products or suffered any adverse reaction/event after use, seek immediate medical advice from a qualified healthcare professional. Healthcare professionals and consumers are advised to report any suspicion of substandard and falsified medicines to NAFDAC.
At EMDEX, we commit to staying true to our vision: Providing Complete, Correct & Current drug and therapeutic information for healthcare professionals.
Our frontline physicians, pharmacists, and nurses have come to rely on EMDEX as the Trusted Source since 1991. EMDEX is used in every Hospital, Clinic & Pharmacy in Nigeria. EMDEX Mobile App currently has 100,000+ downloads!
And each year, we painstakingly update our drug product database.
Are your Pharmaceutical Products registered by NAFDAC? ‘Tis the Season for Enlistment in EMDEX 2023-2024 edition!
Please visit our online portal for information on getting your drug products published in EMDEX Prints & Mobile App
Upskill with our 2-day practice-enhancing workshop specially packaged for the pharmacists including community & hospital pharmacists, Supt or Regulatory Affairs Pharmacists, Product or Marketing Managers, etc.
Taking the quiz will help you identify any knowledge gaps as well as offer you a sneak peek at the course contents. It is free and anonymous, your identity is not collected.
The questions are practice-oriented and completion time estimate is under half an hour. You are strongly encouraged to enroll promptly for the 2-day live workshop if you score below 100%. Seating is limited and filling fast
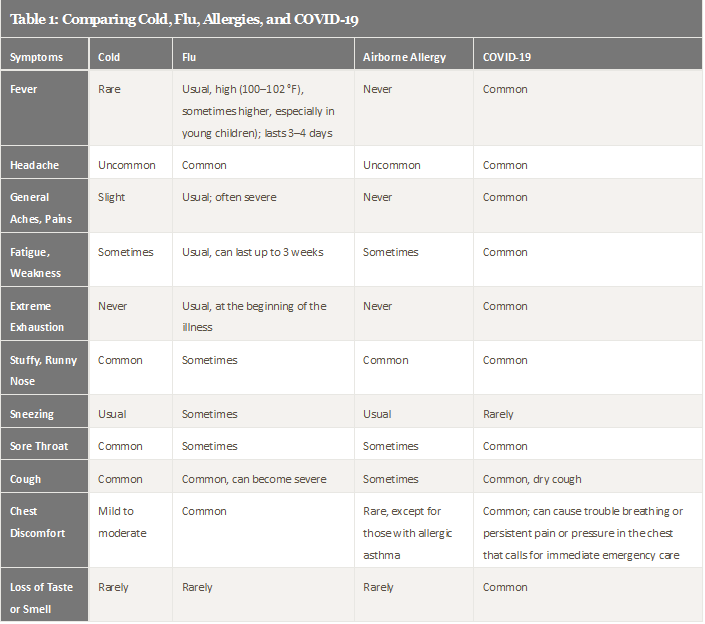
Feeling sick can be especially concerning these days. Could your sniffles be caused by COVID-19? Or the flu? A cold? Or maybe allergies?
Determining the cause of an illness can be tricky because many share some symptoms. They can leave you sniffling, coughing, and feeling tired. But there are important differences.
Figuring out what’s making you sick can help you recover and prevent spreading sickness to others.
See the Comparison Tables 1 & 2 below.
Flu vs COVID-19
“Distinguishing COVID from flu can be difficult because the symptoms overlap so much,” explains Dr. Brooke Bozick, an NIH expert on respiratory diseases that affect the lungs.
Flu and COVID-19 are caused by different viruses that can be spread among people. Flu is caused by the influenza virus. COVID-19 is caused by SARS-CoV-2. Both can give you a fever, cough, headaches, and body aches.
Flu and COVID-19 also spread similarly. They’re transmitted by small particles that come from your nose and mouth when you sneeze, cough, sing, or talk, raising the possibility of infecting people who are nearby. Infected people may not have symptoms, but can still pass along either virus.
“Both influenza and COVID can be spread to other people before individuals develop symptoms,” notes Dr. Aubree Gordon, an infectious disease expert at the University of Michigan.
COVID-19 symptoms can take longer than flu symptoms to develop, she explains. Someone with flu usually has symptoms 1 to 4 days after being infected. A person with COVID-19 typically shows symptoms about 5 days after infection, although this can range from 2 to 14 days.
One telling sign of COVID-19 in some cases is loss of smell or taste. But because of other similar symptoms, there’s really only one way to be certain if you have COVID-19 or flu: Get tested.
Could It Be a Cold? Or Allergies?
Like flu and COVID-19, colds are also caused by viruses and can be passed to others.
Symptoms of a cold tend to be mild. You may have a runny nose, cough, congestion, and sore throat. But you won’t usually have the aches and fever that are common with COVID-19 and flu. Often, you’ll feel better in a couple of days.
There’s no cure for the common cold. Typical treatments include rest, fluids, and over-the-counter medicines. Some complementary treatments may help with cold symptoms, too. Taking honey may help with nighttime cough for children over 1 year old. Rinsing your nose and sinuses can help with congestion. You can use a neti pot or other nasal rinsing device. Be sure to only use water that’s been properly processed, such as distilled or boiled water, not tap water. Nasal rinses can bring relief for both cold and allergies.
Allergies can cause a runny nose and sneezing. But they’re not contagious. If your eyes, nose, or ears itch, that also could be an allergy.
Exposure to things like dust, pets, and tree or grass pollen can trigger allergies, which are caused by the immune system overreacting.
Allergy symptoms tend to stop when you’re no longer exposed to the cause. Unless you have asthma, allergies typically do not cause breathing problems. Allergies can be treated with drugs like antihistamines, decongestants, and nasal steroids.
Wintery Mix of Viruses
Winter is the prime cold and flu season. You’re more likely to be indoors and closer to others when it’s colder outside. Weather also plays a role in the spread of viruses.
“Cold and flu viruses survive better and are more transmissible if it’s cooler and if there’s lower humidity,” Gordon explains.
Experts are concerned that flu and COVID-19 cases may increase and overlap in the winter. Flu cases usually start to increase around October and peak between December and February. Being infected with flu and SARS-CoV-2 at the same time is possible, as is showing symptoms of both.
If you’re sick with the flu, your doctor may prescribe antiviral drugs. Such drugs can make your flu milder and shorten the time you are sick. They work best if they’re used early in your illness.
The FDA has also approved one antiviral drug, called remdesivir, to treat COVID-19. Other treatments are in development and under review. No complementary approaches have been shown to be helpful for fighting off flu or COVID-19.
Fortunately, strategies to prevent the spread of COVID-19 also prevent the spread of flu and cold. “Measures like masking and social distancing work for other respiratory viruses, as well as COVID-19,” says Dr. Chip Walter, who studies vaccine development at Duke University.
Staying Well
There’s another really important way to fight viruses. “Get your flu shot and COVID-19 vaccine,” Walter advises. They are safe and effective ways to protect yourself and those around you.
Don’t forget to vaccinate your children, too. That is the best way to protect their health. COVID-19 vaccines are now recommended for everyone age 5 years and older.
Flu vaccines are recommended for everyone 6 months and older. Flu vaccines are designed to protect against the four types of flu viruses that scientists expect to circulate that year.
Researchers like Walter and others are working to develop flu vaccines that last longer and offer broader protection against many flu strains.
Masks continue to be an important tool for stopping the spread of respiratory viruses, such as COVID-19. “With the pandemic still ongoing, it’s going to be really important that people wear masks,” Gordon says. Try to avoid crowded indoor situations when possible, too.
For more tips on guarding against getting sick this winter, see the Wise Choices below:
Wise Choices
Tips to help you avoid getting sick:
Get a flu shot and COVID-19 vaccine.
Avoid close contact with people who are sick. If you’re sick, limit contact with others to keep from infecting them.
Cover coughs and sneezes. Cover your nose and mouth with a tissue when you cough or sneeze. Throw the tissue in the trash after you use it.
Wash your hands often with soap and water. Scrub your hands for at least 20 seconds. Not sure how long that is? Hum Happy Birthday twice. Be sure to lather the backs of your hands, between your fingers, and under your nails.
Use hand sanitizer if soap and water are not available.
Avoid touching your eyes, nose, and mouth. Germs spread this way.
Clean and disinfect surfaces and objects that may be contaminated with viruses
[National Institutes of Health (NIH) News Bulletin, December 23, 2021] – Chronic infection with the bacterium Helicobacter pylori (H. pylori) is listed as known to be a human carcinogen. This is included in the 15th Report on Carcinogens, bringing the total list to 256 substances that are known, or reasonably anticipated, to cause cancer in humans.
H. pylori is a bacterium that colonizes in the stomach and can cause gastritis and peptic ulcers. Most people do not show symptoms. Chronic infection may lead to stomach cancer and a rare type of stomach lymphoma. Infection primarily occurs from person-to-person contact, especially in crowded housing conditions, and may occur by drinking well water contaminated with H. pylori.
People living in poverty and certain racial, ethnic, and immigrant groups are disproportionately affected by H. pylori infection. Treatment of infected people who have stomach ulcers or signs of stomach infection can decrease their risk of cancer.
Cancer affects almost everyone’s life, either directly or indirectly. As the identification of carcinogens is a key step in cancer prevention, publication of the report represents an important government activity towards improving public health
Rick Woychik, Ph.D., director of the National Institute of Environmental Health Sciences and NTP
The Report on Carcinogens identifies many different environmental factors, collectively called substances, including chemicals; infectious agents, such as viruses; physical agents, such as X-rays and ultraviolet radiation; and exposure scenarios. A substance is listed as either known to be a human carcinogen or reasonably anticipated to be a human carcinogen, to indicate the potential hazard.
The report does not include estimates of cancer risk because many factors affect whether a person will or will not develop cancer. Those include the carcinogenic potency of the substance, the level and duration of exposure, and an individual’s susceptibility to the carcinogenic action of the substance.
[WHO Update, 28 November 2021] – On 26 November 2021, WHO designated the variant B.1.1.529 a variant of concern, named Omicron, on the advice of WHO’s Technical Advisory Group on Virus Evolution (TAG-VE). This decision was based on the evidence presented to the TAG-VE that Omicron has several mutations that may have an impact on how it behaves, for example, on how easily it spreads or the severity of illness it causes.
Here is a summary of what is currently known.
Current knowledge about Omicron
Researchers in South Africa and around the world are conducting studies to better understand many aspects of Omicron and will continue to share the findings of these studies as they become available.
Transmissibility: It is not yet clear whether Omicron is more transmissible (e.g., more easily spread from person to person) compared to other variants, including Delta. The number of people testing positive has risen in areas of South Africa affected by this variant, but epidemiologic studies are underway to understand if it is because of Omicron or other factors.
Severity of disease: It is not yet clear whether infection with Omicron causes more severe disease compared to infections with other variants, including Delta. Preliminary data suggests that there are increasing rates of hospitalization in South Africa, but this may be due to increasing overall numbers of people becoming infected, rather than a result of specific infection with Omicron. There is currently no information to suggest that symptoms associated with Omicron are different from those from other variants. Initial reported infections were among university studies—younger individuals who tend to have more mild disease—but understanding the level of severity of the Omicron variant will take days to several weeks. All variants of COVID-19, including the Delta variant that is dominant worldwide, can cause severe disease or death, in particular for the most vulnerable people, and thus prevention is always key.
Effectiveness of prior SARS-CoV-2 infection
Preliminary evidence suggests there may be an increased risk of reinfection with Omicron (i.e., people who have previously had COVID-19 could become reinfected more easily with Omicron), as compared to other variants of concern, but information is limited. More information on this will become available in the coming days and weeks.
Effectiveness of vaccines: WHO is working with technical partners to understand the potential impact of this variant on our existing countermeasures, including vaccines. Vaccines remain critical to reducing severe disease and death, including against the dominant circulating virus, Delta. Current vaccines remain effective against severe disease and death.
Effectiveness of current tests: The widely used PCR tests continue to detect infection, including infection with Omicron, as we have seen with other variants as well. Studies are ongoing to determine whether there is any impact on other types of tests, including rapid antigen detection tests.
Effectiveness of current treatments: Corticosteroids and IL6 Receptor Blockers will still be effective for managing patients with severe COVID-19. Other treatments will be assessed to see if they are still as effective given the changes to parts of the virus in the Omicron variant.
Studies underway
At the present time, WHO is coordinating with a large number of researchers around the world to better understand Omicron. Studies currently underway or underway shortly include assessments of transmissibility, severity of infection (including symptoms), performance of vaccines and diagnostic tests, and effectiveness of treatments.
WHO encourages countries to contribute the collection and sharing of hospitalized patient data through the WHO COVID-19 Clinical Data Platform to rapidly describe clinical characteristics and patient outcomes.
More information will emerge in the coming days and weeks. WHO’s TAG-VE will continue to monitor and evaluate the data as it becomes available and assess how mutations in Omicron alter the behaviour of the virus.
Recommended actions for countries
As Omicron has been designated a Variant of Concern, there are several actions WHO recommends countries to undertake, including enhancing surveillance and sequencing of cases; sharing genome sequences on publicly available databases, such as GISAID; reporting initial cases or clusters to WHO; performing field investigations and laboratory assessments to better understand if Omicron has different transmission or disease characteristics, or impacts effectiveness of vaccines, therapeutics, diagnostics or public health and social measures. More detail in the announcement from 26 November.
Countries should continue to implement the effective public health measures to reduce COVID-19 circulation overall, using a risk analysis and science-based approach. They should increase some public health and medical capacities to manage an increase in cases. WHO is providing countries with support and guidance for both readiness and response.
In addition, it is vitally important that inequities in access to COVID-19 vaccines are urgently addressed to ensure that vulnerable groups everywhere, including health workers and older persons, receive their first and second doses, alongside equitable access to treatment and diagnostics.
Recommended actions for people
The most effective steps individuals can take to reduce the spread of the COVID-19 virus is to keep a physical distance of at least 1 metre from others; wear a well-fitting mask; open windows to improve ventilation; avoid poorly ventilated or crowded spaces; keep hands clean; cough or sneeze into a bent elbow or tissue; and get vaccinated when it’s their turn.
WHO will continue to provide updates as more information becomes available, including following meetings of the TAG-VE. In addition, information will be available on WHO’s digital and social media platforms.
[WHO Statement, 26 November 2021] – The Technical Advisory Group on SARS-CoV-2 Virus Evolution (TAG-VE) is an independent group of experts that periodically monitors and evaluates the evolution of SARS-CoV-2 and assesses if specific mutations and combinations of mutations alter the behaviour of the virus. The TAG-VE was convened on 26 November 2021 to assess the SARS-CoV-2 variant: B.1.1.529.
The B.1.1.529 variant was first reported to WHO from South Africa on 24 November 2021. The epidemiological situation in South Africa has been characterized by three distinct peaks in reported cases, the latest of which was predominantly the Delta variant. In recent weeks, infections have increased steeply, coinciding with the detection of B.1.1.529 variant. The first known confirmed B.1.1.529 infection was from a specimen collected on 9 November 2021.
This variant has a large number of mutations, some of which are concerning. Preliminary evidence suggests an increased risk of reinfection with this variant, as compared to other VOCs. The number of cases of this variant appears to be increasing in almost all provinces in South Africa. Current SARS-CoV-2 PCR diagnostics continue to detect this variant. Several labs have indicated that for one widely used PCR test, one of the three target genes is not detected (called S gene dropout or S gene target failure) and this test can therefore be used as marker for this variant, pending sequencing confirmation. Using this approach, this variant has been detected at faster rates than previous surges in infection, suggesting that this variant may have a growth advantage.
There are a number of studies underway and the TAG-VE will continue to evaluate this variant. WHO will communicate new findings with Member States and to the public as needed.
Based on the evidence presented indicative of a detrimental change in COVID-19 epidemiology, the TAG-VE has advised WHO that this variant should be designated as a VOC, and the WHO has designated B.1.1.529 as a VOC, named Omicron.
As such, countries are asked to do the following:
enhance surveillance and sequencing efforts to better understand circulating SARS-CoV-2 variants.
submit complete genome sequences and associated metadata to a publicly available database, such as GISAID.
report initial cases/clusters associated with VOC infection to WHO through the IHR mechanism.
where capacity exists and in coordination with the international community, perform field investigations and laboratory assessments to improve understanding of the potential impacts of the VOC on COVID-19 epidemiology, severity, effectiveness of public health and social measures, diagnostic methods, immune responses, antibody neutralization, or other relevant characteristics.
Individuals are reminded to take measures to reduce their risk of COVID-19, including proven public health and social measures such as wearing well-fitting masks, hand hygiene, physical distancing, improving ventilation of indoor spaces, avoiding crowded spaces, and getting vaccinated.
The US Centers for Disease Control and Prevention recommends COVID-19 vaccination for all people aged 12 years and older, including people who are pregnant, breastfeeding, trying to get pregnant now, or might become pregnant in the future. Pregnant and recently pregnant people are more likely to get severely ill with COVID-19 compared with non-pregnant people. Getting a COVID-19 vaccine can protect you from severe illness from COVID-19.
If you are pregnant, you might want to have a conversation with your healthcare provider about COVID-19 vaccination. While such a conversation might be helpful, it is not required before vaccination. You can receive a COVID-19 vaccine without any additional documentation from your healthcare provider.
If you got pregnant after receiving your first shot of a COVID-19 vaccine that requires two doses (i.e., Pfizer-BioNTech COVID-19 vaccine or Moderna COVID-19 vaccine), you should get your second shot to get as much protection as possible. If you experience fever following vaccination, you should take paracetamol (EASADOL®) because fever—for any reason—has been associated with adverse pregnancy outcomes.
Recommendations for breastfeeding mom
COVID-19 vaccination is recommended for all people 12 years and older, including people who are breastfeeding. Clinical trials for the COVID-19 vaccines currently used in the United States did not include people who are breastfeeding. Because the vaccines have not been studied in people who are breastfeeding, there are limited data available on the:
Safety of COVID-19 vaccines in people who are breastfeeding
Effects of vaccination on the breastfed baby
Effects on milk production or excretion
COVID-19 vaccines cannot cause infection in anyone, including the mother or the baby, and the vaccines are effective at preventing COVID-19 in people who are breastfeeding. Recent reports have shown that breastfeeding people who have received mRNA COVID-19 vaccines have antibodies in their breastmilk, which could help protect their babies. More data are needed to determine what protection these antibodies may provide to the baby.